
Abstract
Summary: Pituitary apoplexy is defined as a clinical syndrome that may include headache, visual deficits, ophthalmoplegia, or altered mental status. It may result from either infarction or hemorrhage of the pituitary gland. Prognosis is significantly improved with early diagnosis and surgical treatment. We report two cases in which diffusion-weighted MR imaging assisted in the early detection of acute pituitary infarction and led, in one case, to surgical intervention early in the course of clinical apoplexy, with resulting complete recovery.
Pituitary apoplexy may have a variable clinical presentation but should be suspected in any patient with severe headache, visual deficits, ophthalmoplegia, or altered mental status. Symptoms may progress over weeks or occur abruptly and lead to coma and death (1). Apoplexy commonly occurs with a preexisting pituitary adenoma (2). Routine MR imaging may be useful for the detection of pituitary hemorrhage, especially in the subacute setting (2), but hemorrhage is not an essential element, because clinical apoplexy can occur in the setting of bland pituitary infarction (3). Previous reports have suggested that pituitary infarction may be predicted by the presence of peripheral contrast enhancement of an intrasellar mass on MR images (3, 4). This appearance, however, is not specific and may be present in association with cystic pituitary adenoma and craniopharyngioma. We report two cases in which restricted water diffusion within pituitary adenomas indicated the onset of clinical apoplexy in one patient and led to early surgical intervention in a second patient before the onset of clinical apoplexy.
Case Reports
Patient 1
A 57-year-old man with a medical history of hypertension and hypercholesterolemia presented with sudden-onset blurred vision in the right eye that he described as being like “a curtain coming up” over the eye. This was initially associated with headache and nausea, but symptoms had partially resolved by the time the patient arrived at the emergency department. He denied paresthesias or weakness. A physical examination revealed an inferior temporal quadrantopsia but otherwise normal physical and neurologic results. Non-enhanced CT (Fig 1A) showed a 1.5-cm noncystic homogeneous intrasellar mass without evidence of hemorrhage. Although the initial diagnosis included pituitary apoplexy, amaurosis fugax was considered to be more likely because of improving symptoms. Emergent MR imaging (Fig 1B and C) and MR angiography showed a homogeneous intrasellar mass that did not enhance or contain hemorrhage. Cervical MR angiography showed normal flow pattern of the carotid bifurcations. The next morning, the patient’s vision was stable, and elective resection of the pituitary tumor was planned. That afternoon, the patient reported sudden complete vision loss in the left eye. He was immediately taken to surgery, where transphenoidal resection of a pituitary macroadenoma was performed. Histologic analysis revealed the presence of a necrotic pituitary adenoma with hemorrhage. Immediately after surgery, light perception returned to the left eye with 20/40 vision in the right eye. The patient developed mild adrenal and thyroid insufficiency, requiring hormonal replacement. He was eventually discharged home with a persistent but slowly improving left eye visual defect.
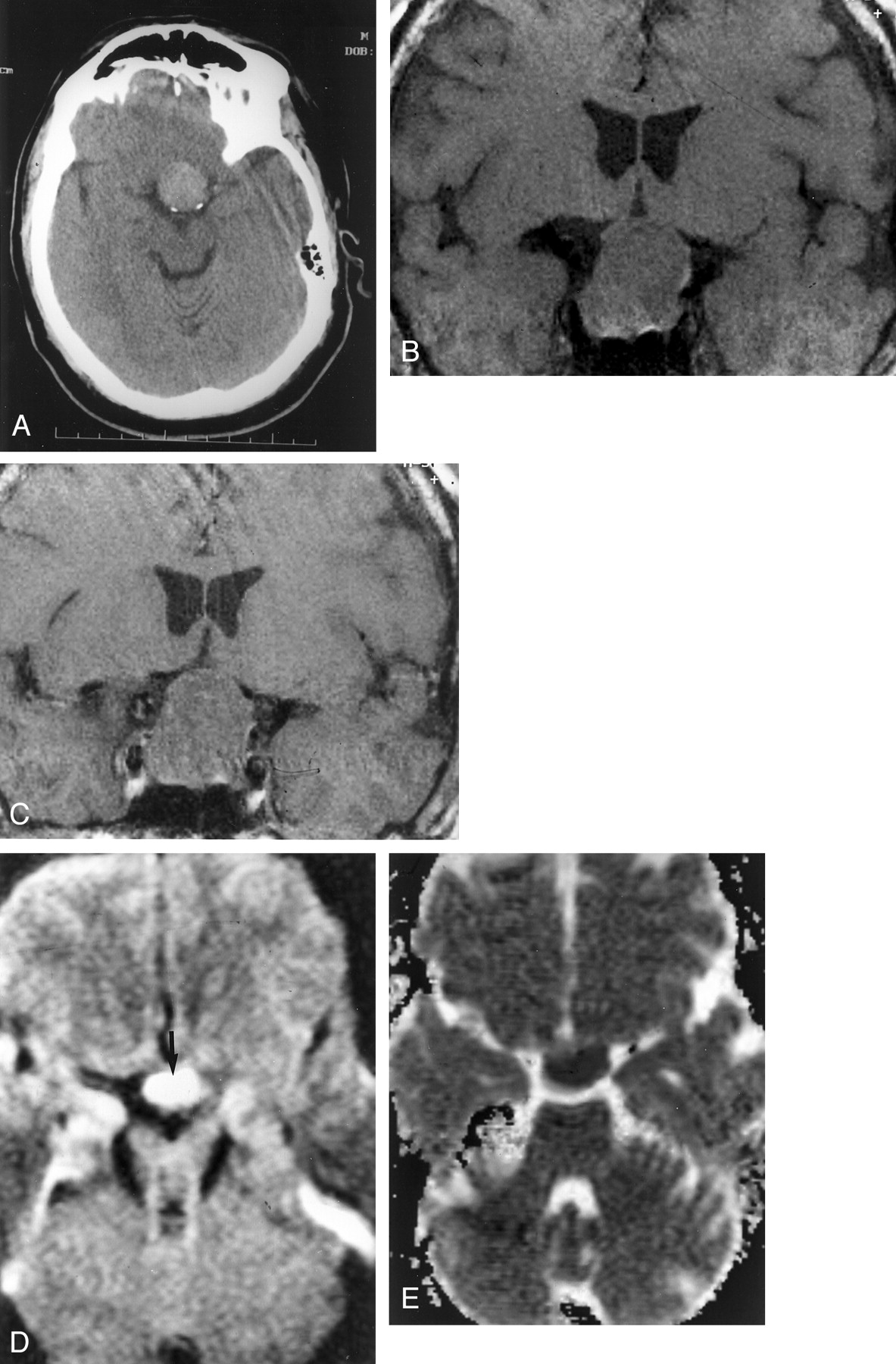
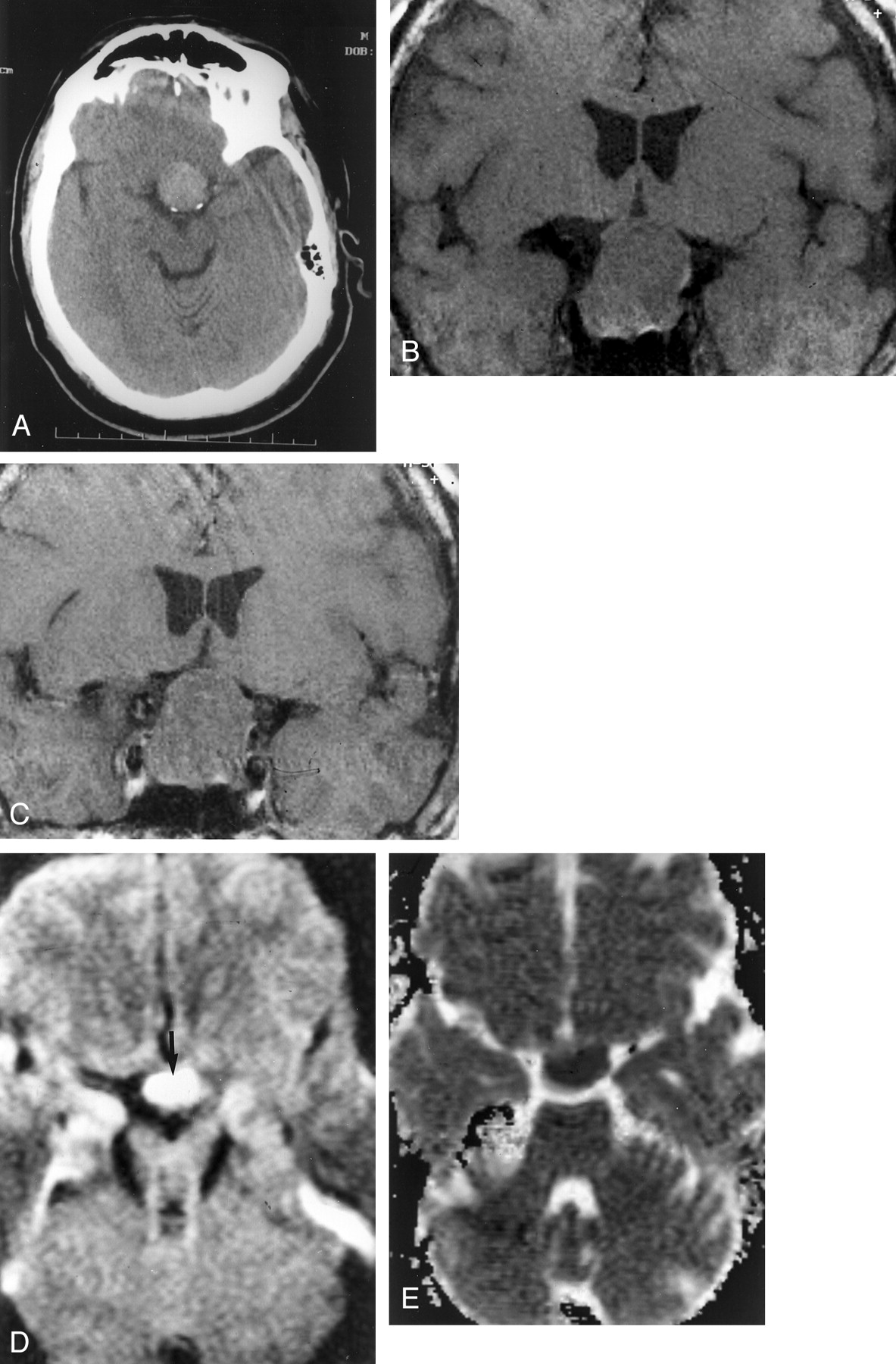
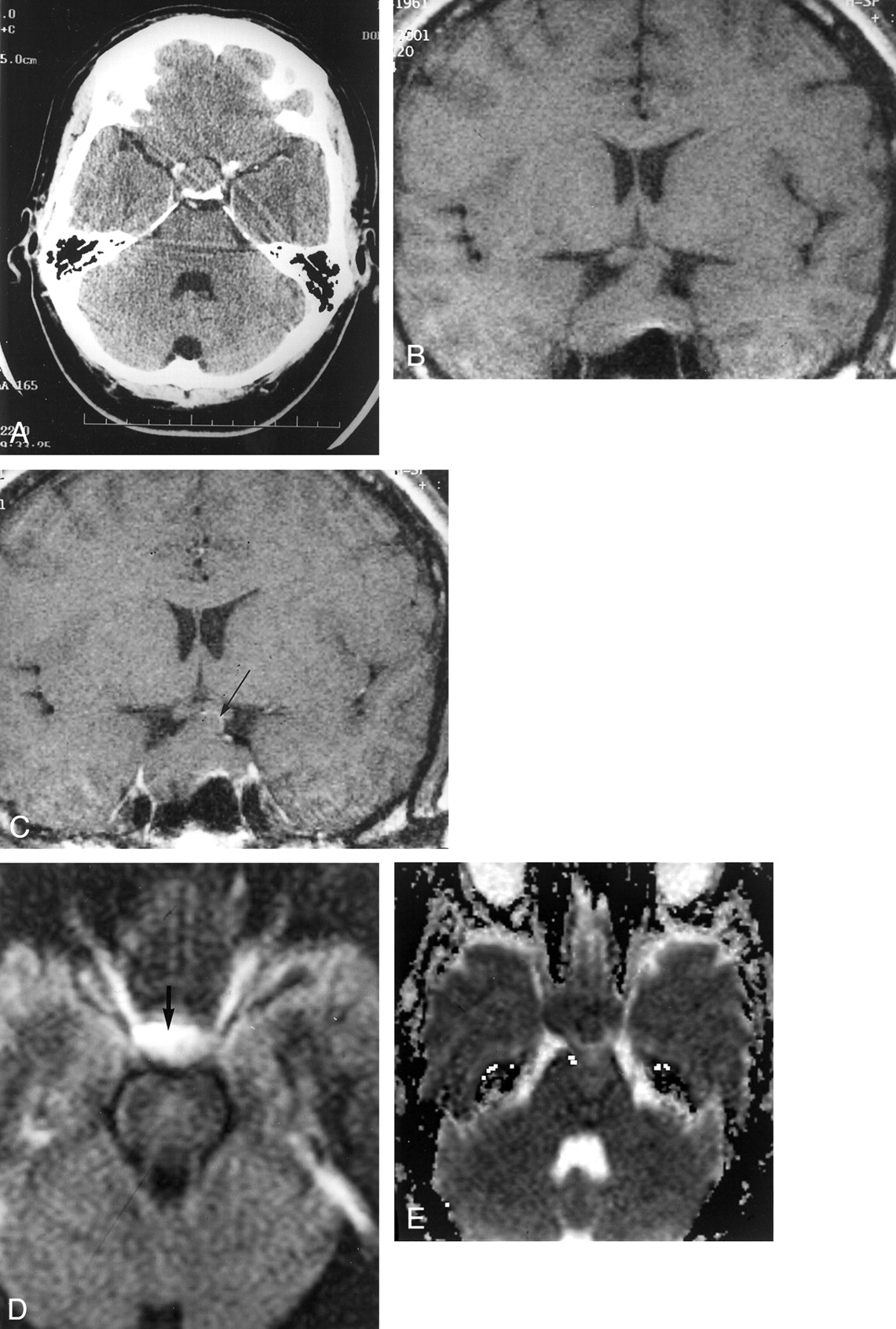
The case of a 57-year-old man who presented with decreased vision in his right eye.
A, Nonenhanced CT scan shows a homogeneous, nonhemorrhagic, hyperattenuated intrasellar mass.
B, Coronal spin-echo T1-weighted MR image (500/20 [TR/TE]) shows a large homogeneous intrasellar mass that compresses the optic chiasm, consistent with a nonhemorrhagic macroadenoma.
C, Coronal spin-echo T1-weighted MR image (500/20) shows no change after the administration of contrast medium (0.05 mmol/kg).
D, Tensor diffusion-weighted MR image (b = 1000 mm2/s) shows markedly increased signal intensity (arrow) within the pituitary mass, compared with that in normal gray and white matter.
E, ADC map shows markedly decreased signal intensity within the pituitary mass; mean ADC was 0.49 (10–3 mm2/s).
A retrospective review showed the tensor axial diffusion-weighted MR images of the adenoma to be hyperintense relative to normal gray and white matter (Fig 1D), with decreased signal intensity on the apparent diffusion coefficient (ADC) map (Fig 1E). The calculated ADC value was 0.49 (10–3 mm2/s), consistent with restricted diffusion.
Patient 2
A 40-year-old man with a medical history of hypercholesterolemia awoke with severe bilateral retro-orbital pain. His headache was not associated with visual changes, weakness, or seizure. At the emergency department, he was noted to have intact visual fields and normal results of a neurologic examination. Contrast-enhanced CT revealed a large nonenhancing intrasellar mass (Fig 2A), with no evidence of hemorrhage. Emergent MR imaging was performed and showed a homogeneous intrasellar mass with minimal linear peripheral contrast enhancement and no evidence of hemorrhage (Fig 2B and C). Evaluation of the tensor diffusion-weighted MR images (Fig 2D) showed the mass to be hyperintense relative to normal gray and white matter, with hypointensity on the ADC map (Fig 2E). The calculated ADC value was 0.63 10–3 mm2/s, consistent with restricted diffusion. Pituitary infarction was diagnosed on the basis of these findings. Emergent transphenoidal surgery was performed within 48 hours of presentation. Surgical resection revealed infarcted pituitary adenoma with areas of gross necrosis. The patient had an uneventful postoperative course and was discharged home with no residual neurologic deficits.
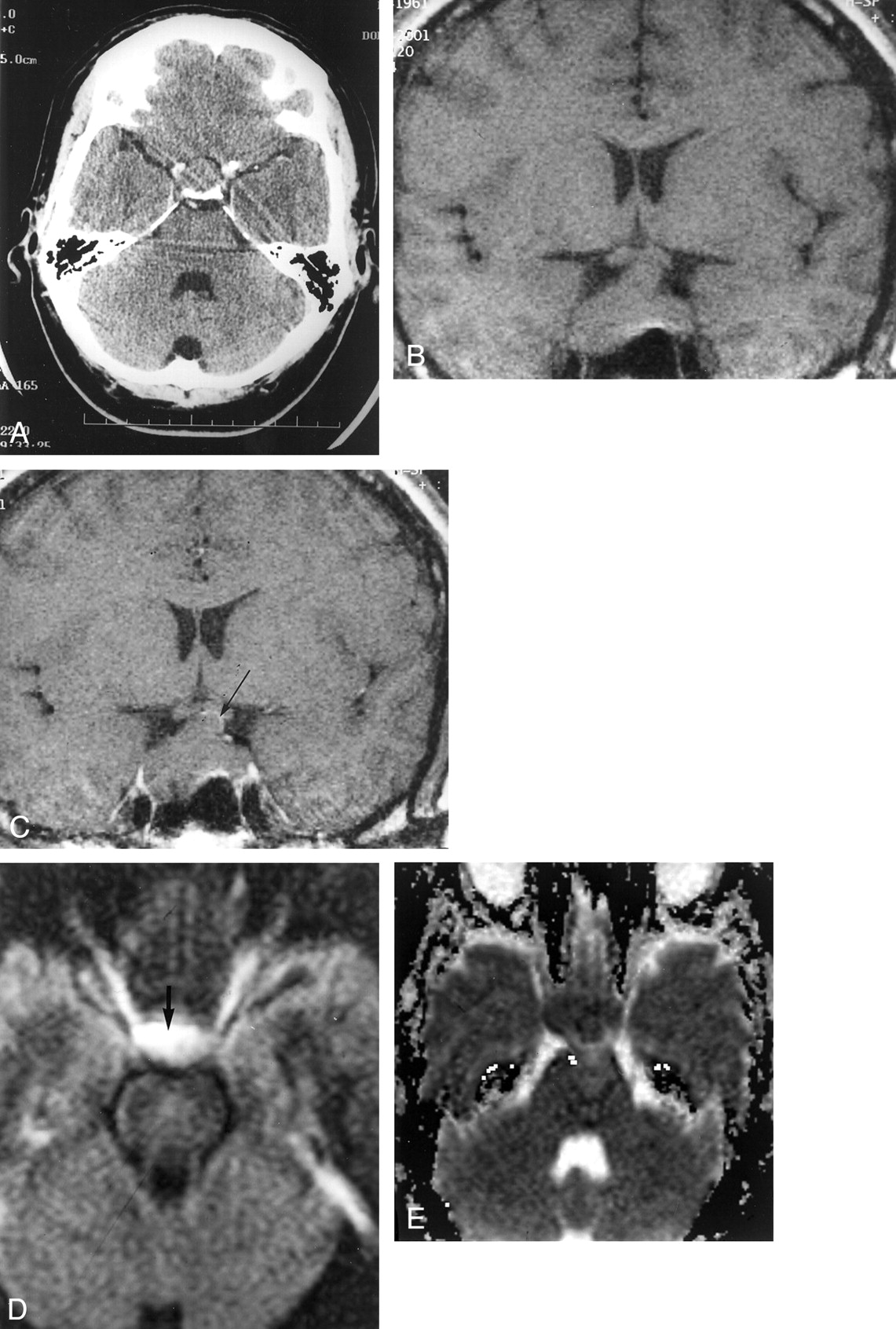
The case of a 40-year-old man who awoke with severe bilateral retro-orbital pain.
A, Axial contrast-enhanced CT scan shows a nonenhancing homogeneous intrasellar mass. No hemorrhage is seen.
B, Coronal spin-echo T1-weighted MR image (500/20 [TR/TE]) shows a nonhemorrhagic intrasellar mass with extension to the optic chiasm.
C, Coronal spin-echo T1-weighted MR image (500/20) shows minimal curvilinear marginal enhancement (arrow) after the administration of contrast medium (0.05 mmol/kg).
D, Tensor diffusion-weighted MR image (b = 1000 mm2/s) shows increased signal intensity (arrow) within the pituitary mass, compared with that in normal gray and white matter.
E, ADC map shows decreased signal intensity within the pituitary mass; mean ADC was 0.63 (10–3 mm2/s).
Discussion
Early diagnosis and treatment of pituitary apoplexy is necessary if significant associated morbidity and mortality are to be prevented. Although the clinical presentation may vary in terms of the nature, onset, and progression of symptoms, the diagnosis should be considered for any patient presenting with headache, visual field deficits, ophthalmoplegia, or altered mental status (3). Apoplexy may result from either pituitary infarction or hemorrhage (3). Clinical risk factors are trauma, increased intracranial pressure, anticoagulation, bromocriptine therapy, diabetic ketoacidosis, conventional angiography, radiation therapy, and open heart surgery (4).
Although tumor regression has been reported after conservative management of apoplexy due to nonhemorrhagic infarction of pituitary macroadenoma (4), this treatment is generally selected only in cases in which concurrent medical illness contraindicates surgery. A recent retrospective study reports that surgery resulted in improvements in visual acuity, visual field defects, and ocular paresis in 88%, 95%, and 100%, respectively, of patients with pituitary apoplexy. Early surgical intervention was therefore recommended (2).
MR imaging of pituitary macroadenomas generally shows early contrast enhancement because of a direct arterial supply to the tumor, but enhancement may vary in homogeneity and intensity depending on the histologic composition of the tumor (5). Peripheral enhancement has been described as a sign of macroadenoma infarction in both acute and chronic settings (3, 6). This MR imaging appearance was found to correspond to the presence of granulation tissue and lymphocytosis at histologic examination. Minimal peripheral contrast enhancement was present in one of the cases presented herein; however, peripheral enhancement is not specific for infarction, because it can be seen in association with cystic macroadenoma and craniopharyngioma. The absence of contrast enhancement in cases of pituitary infarction has not, as far as we can determine, been previously described and may result from a combination of decreased perfusion and tumor necrosis.
To our knowledge, the use of diffusion-weighted MR imaging has not been previously reported for the diagnosis of pituitary adenoma with infarction. Although we know of no published data concerning expected ADC values for noninfarcted pituitary adenoma, restricted diffusion would not be an expected finding. Low absolute and relative ADC values have been reported to occur in association with high-grade brain tumors; it seems that an inverse correlation exists between tumor cellularity and water diffusion (7). The two cases presented herein show histologically typical benign pituitary macroadenoma without a high nuclear-cytoplasmic ratio or attenuated cellularity and therefore would not be expected to show restricted diffusion. This premise is supported by two additional cases (Figs 3 and 4) of histologically confirmed, noninfarcted macroadenoma. In both of these cases, tensor and ADC images appeared nearly isointense to normal brain parenchyma on diffusion-weighted MR images. The calculated ADC value available for one of these adenomas (Fig 4) was 0.90 (10–3 mm2/s), similar to that measured in normal brain parenchyma, in this case, from temporal lobe white matter at 1.1 (10–3 mm2/s). Findings in this limited sample support the expected absence of diffusion restriction in the noninfarcted pituitary adenoma.

The case of a 64-year-old man with histologically confirmed pituitary adenoma without evidence of hemorrhage or infarction.
A, Coronal spin-echo T1-weighted MR image (500/20 [TR/TE]) shows a large homogeneous intrasellar mass compressing the optic chasm, consistent with a nonhemorrhagic macroadenoma.
B, Coronal spin-echo T1-weighted MR image (500/20) shows diffuse uniform enhancement after the administration of contrast medium (0.05 mmol/kg).
C and D, Tensor diffusion-weighted MR images (b = 1000 mm2/s) show isointensity within the pituitary mass (arrows) compared with that in normal brain.
E and F, ADC maps show isointensity within the pituitary mass (arrows) compared with that in normal brain.
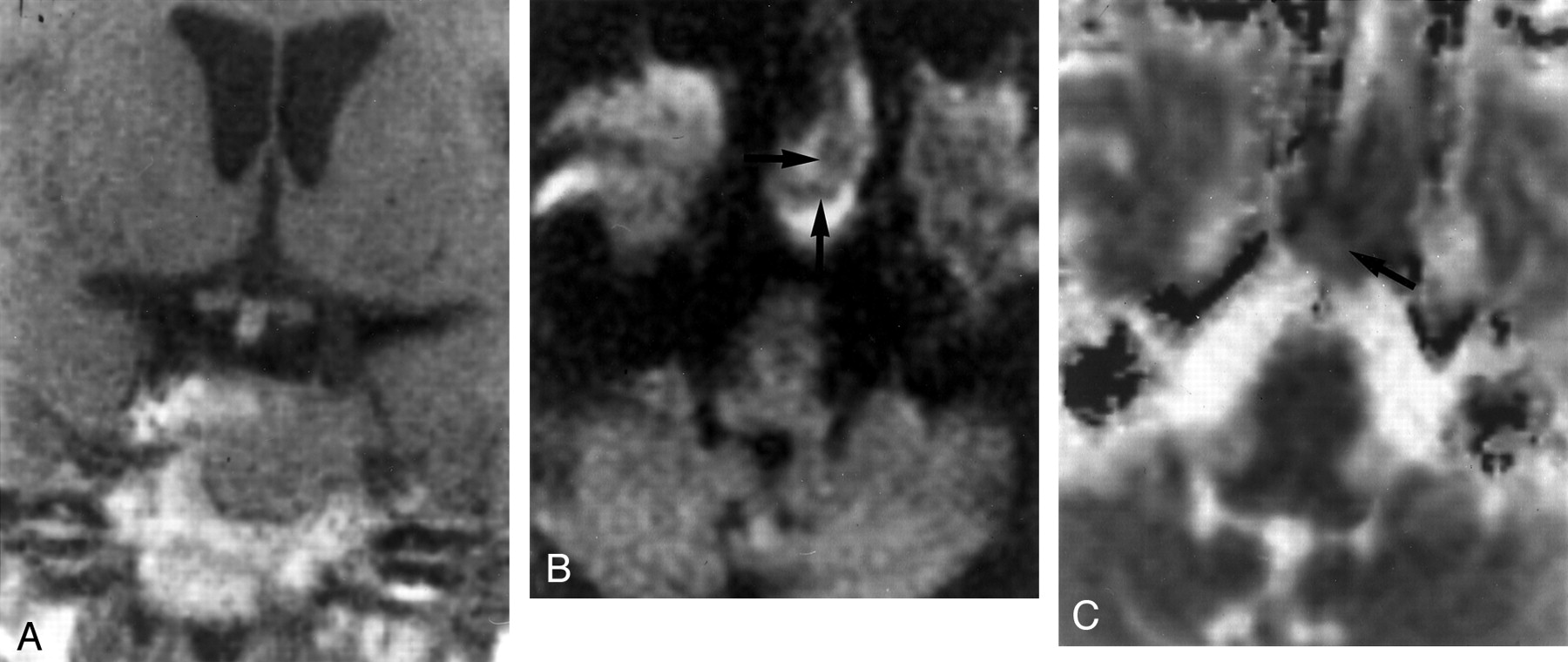
The case of a 69-year-old woman with histologically confirmed pituitary adenoma without evidence of hemorrhage or infarction.
A, Coronal spin-echo T1-weighted MR image (500/20 [TR/TE]) shows a homogeneous intrasellar mass extending inferiorly, with remodeling of the sellar floor.
B, Tensor diffusion-weighted MR image (b = 1000 mm2/s) shows isointensity within the pituitary mass (arrows) compared with that in normal brain.
C, ADC map shows isointensity within the pituitary mass (arrow) compared with that in normal brain; mean ADC was 0.90 (10–3 mm2/s).
Restricted water diffusion is an accepted sign of acute cerebral infarction. In cases of ischemic infarction, decreased proton mobility results from increased intracellular water and diminished extracellular space caused by sodium-potassium pump failure (8). These same mechanisms are likely responsible for the restricted diffusion in the two cases presented herein. An alternate explanation for restricted diffusion is the presence of tumor necrosis. Restricted diffusion in a cerebral mass with necrosis has been recently reported (9). Restricted diffusion was attributed to the presence of liquifactive necrosis that may have a puslike matrix and diffusion characteristics comparable with those of intracranial abscess.
Possible differential diagnoses for the presented cases based on diffusion MR imaging findings are pituitary hemorrhage, abscess, and hypophysitis. Pituitary hemorrhage, which was not shown on images at presentation in either of the two cases reported herein, could result in restricted diffusion in the absence of infarction resulting from the effect of acute intracellular blood products on proton diffusion (10). Differentiation of pituitary infarction from infection may be difficult. Although pituitary infection is rare, clinical manifestations of infection may be absent. The intrasellar mass will typically show peripheral enhancement surrounding a hypointense core (11) that may mimic infarction. Restricted diffusion within an abscess is also well described (12). The diffusion imaging characteristics of pituitary lymphocytic hypophysitis have not yet been described, as far as we can determine. Lymphocytic hypophysitis is a noninfectious inflammatory process in which the pituitary is infiltrated by lymphocytes and plasma cells. Although one may suspect that the inflammatory nature of this process can result in restricted diffusion and that the imaging appearance can mimic macroadenoma, the clinical picture is fairly specific and should be suspected primarily in women who are either pregnant or recently postpartum (11).
Conclusion
We present the case reports of two patients with clinically acute pituitary apoplexy in which restricted diffusion on MR images and a lack of contrast enhancement indicated the presence of pituitary infarction and, in one case, resulted in early surgical intervention with excellent outcome.
References
- Received November 16, 2001.
- Accepted after revision March 19, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pituitary tumour apoplexy due to pituitary adenoma in a dog: clinical, 3T MRI and CT features
- Intravoxel Incoherent Motion in Normal Pituitary Gland: Initial Study with Turbo Spin-Echo Diffusion-Weighted Imaging
- Evaluation of Diffusivity in the Anterior Lobe of the Pituitary Gland: 3D Turbo Field Echo with Diffusion-Sensitized Driven-Equilibrium Preparation