
Abstract
Summary: Astroblastoma is a rare primary glial tumor with a characteristic appearance on neuroradiologic images. Typically, astroblastomas are large, lobulated, peripheral, supratentorial, solid, and cystic masses with relatively little associated vasogenic edema and tumor infiltration for their large size. The solid component of the mass has a bubbly appearance and a T2 signal that is isointense to gray matter. Punctate calcifications are often present. Neuroradiologists should be familiar with the characteristic appearance of this tumor.
Astroblastoma is a rare glial tumor estimated to account for 0.45–2.8% of primary brain gliomas (1). These tumors were initially described by Bailey and Cushing (2) and further characterized by Bailey and Bucy (3); however, in the following decades much confusion has arisen regarding criteria for their diagnosis. In addition, the cell of origin of these tumors has been debated, because they share features of both astrocytomas and ependymomas. Recent histopathologic and comparative genomic findings have suggested that astroblastoma is indeed a distinct entity (4). We tested the hypothesis that neuroradiologic features might be helpful in distinguishing astroblastomas from other tumors that are often confused with them.
Case Reports
We performed a retrospective analysis of CT and MR images obtained from six patients with pathologically confirmed astroblastoma. The Table depicts patient demographics; patients ranged in age from 3–46 years (mean, 20.5 years); five were female, and one was male.
Patient Demographics
Astroblastomas and ependymomas have a similar histologic appearance characterized by a radiating arrangement of spindle-shaped tumor cells forming perivascular pseudorosettes. These pseudorosettes are similar to those seen in ependymomas, and histopathologic distinction between these two entities is often difficult. Distinctive histologic features of astroblastoma, such as broad tapering cellular processes extending to central vessels, perivascular hyalinization, and lack of fibrillarity, can help the pathologist discriminate between the two tumors. However, both astroblastoma and ependymoma have anaplastic or “malignant” counterparts, characterized by higher cellularity and proliferation, necrosis, and vascular proliferation; in these cases, distinguishing between the two tumor types can be impossible (Fig 1).

Histopathologic specimens of a well-differentiated and malignant astroblastoma.
A, Well-differentiated astroblastomas are composed of astroblastic pseudorosettes, which are elongated tumor cells with broad or tapering processes extending to a central vessel (arrow).
B, Malignant astroblastomas contain hypercellular mitotically active regions that often display vascular proliferation or necrosis (arrowheads).
On MR images, the classic appearance of astroblastoma is that of a large, well-circumscribed, lobulated peripheral mass in the supratentorial brain (Figs 2–4). The mass typically consists of a mixture of cystic and solid components; the latter exhibits a heterogeneous bubbly appearance on T2-weighted images. The solid portions of the masses are relatively hypointense to gray matter on T1-weighted images and isointense to gray matter on T2-weighted images. Given the large size of the masses, a relative lack of peritumoral T2 hyperintensity exists, representing vasogenic edema or tumor infiltration or both in the surrounding brain parenchyma. Enhancement is heterogeneous, with rim enhancement of the cystic portion and heterogeneous enhancement of the solid portion. CT occasionally depicts punctate calcifications within the solid portion of these tumors; the solid portion can also appear hyperattenuated.

The classic MR imaging appearance of an astroblastoma in a 3-year-old female patient (patient 5).
A and B, Axial T2-weighted images [2500/90/1 (TR/TE/excitations)] depict a large, well-circumscribed, heterogeneous supratentorial mass with peripheral cystic changes (arrows). Note that the solid component of the mass has a heterogeneous bubbly appearance in its center.
C and D, Axial postcontrast T1-weighted images (500/20/1) show rim enhancement of the cystic component (arrows) and heterogeneous enhancement of the solid component. In this case, the tumor was malignant.
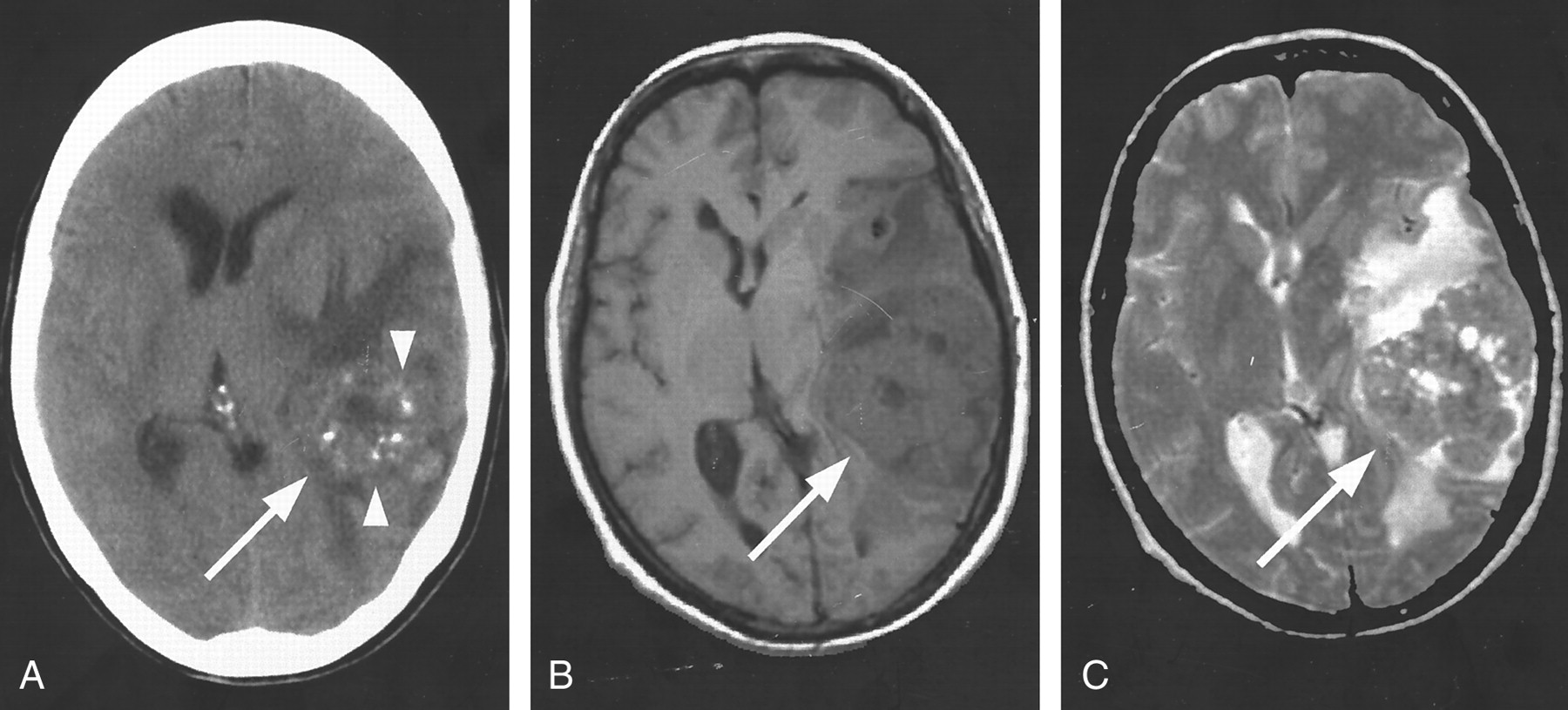
The classic CT and MR imaging appearance of an astroblastoma in a 42-year-old female patient (patient 2).
A, Axial non-contrast-enhanced CT scan shows punctate calcifications (arrowheads) within the solid portion of the large left temporal lobe mass (arrow).
B, Axial non-contrast-enhanced T1-weighted image (500/8/1) shows the solid portion of the tumor (arrow) to be relatively hypointense to gray matter.
C, Axial T2-weighted image (2640/98/1) shows the solid portion of the tumor (arrow) as isointense to gray matter. This tumor was well differentiated.
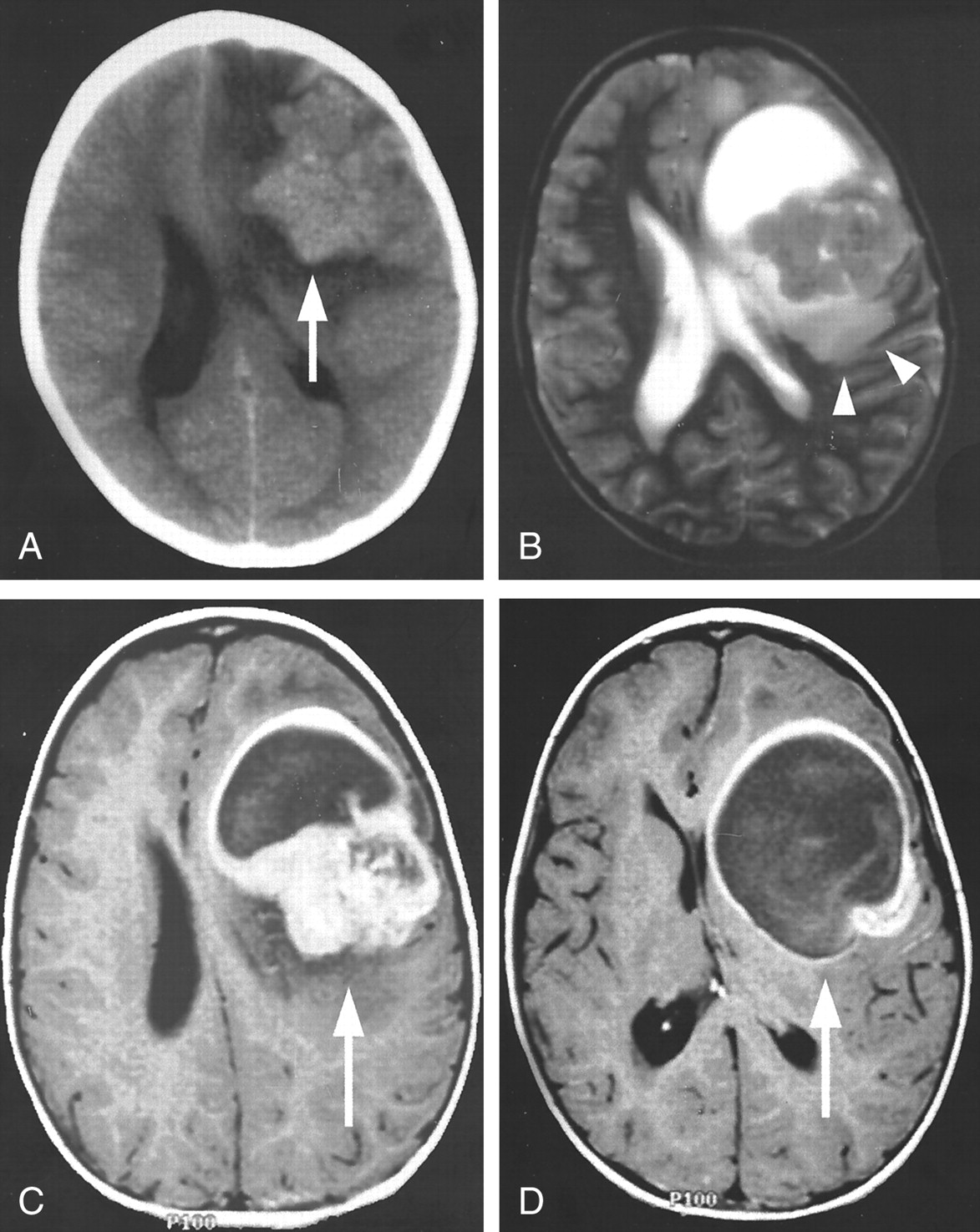
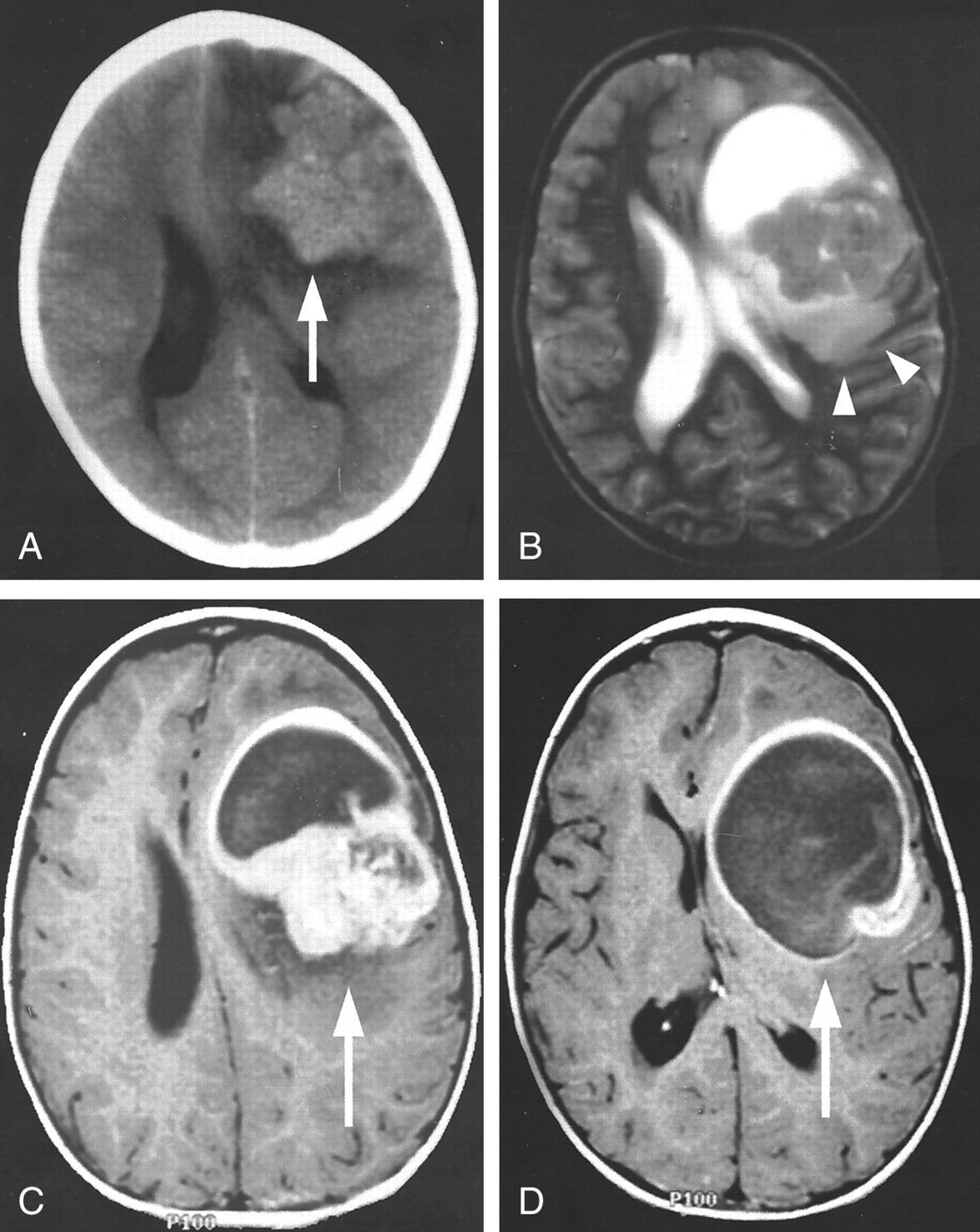
The classic CT and MR imaging appearance of an astroblastoma in a 5-year-old female patient (patient 4).
A, Axial non-contrast-enhanced CT scan shows the solid component of the mass has a slightly higher attenuation than that of the adjacent gray matter (arrow).
B, Axial T2-weighted image (7935/115/1) depicts the relative lack of peritumoral T2 hyperintensity (representing vasogenic edema or tumor infiltration or both) given the large tumor size (arrowheads).
C and D, Axial postcontrast T1-weighted images (450/18/1) depict intense heterogeneous enhancement of the solid portion (C, arrow) and rim enhancement of the cystic portion (D, arrow). The diagnosis of a malignant astroblastoma was confirmed on the basis of histologic findings.
Usually no radiographic distinction is evident between well-differentiated and malignant astroblastomas. Infrequently, however, malignant astroblastomas may be aggressive (Fig 5). Features such as invasion of the corpus callosum may suggest the diagnosis of ependymoma; however, the supratentorial location, relative lack of vasogenic edema, tumor infiltration for the size of the mass, and the somewhat bubbly appearance of the solid portion are unusual findings for ependymoma and favor astroblastoma.

MR images of an aggressive astroblastoma in a 15-year-old female patient (patient 6).
A, Sagittal T1-weighted image (810/14/1) shows an aggressive mass that has invaded the anterior body of the corpus callosum (arrowhead).
B, Axial T2-weighted image (5000/93/1) shows the lesion to have slightly higher T2 signal intensity than that typically seen with an astroblastoma, and the mass appears centered within the anterior horn of the left lateral ventricle (arrow), suggesting the diagnosis of ependymoma.
C, Coronal postcontrast T1-weighted image (950/14/1) depicts heterogeneous enhancement of the solid portion (arrowhead) and rim enhancement around the cystic portion (arrow). The tumor was a malignant astroblastoma.
Distinction from ependymoma and other tumors can be difficult when the lesions are small (Fig 6). Our two cases of well-differentiated, relatively small astroblastomas (<3-cm maximum diameter, patients 1 and 3) showed a moderate amount of associated peritumoral T2 hyperintensity; the exact reason for this finding is unclear. However, both of these small tumors exhibited the other characteristics of astroblastomas, namely, they were well-circumscribed, lobulated, peripheral masses in the supratentorial brain with a mixture of cystic and bubbly solid components.

MR images of a relatively small astroblastoma in a 30-year-old male patient (patient 1).
A, Axial T2-weighted image (3466/84/1) shows the solid component of this left frontal lesion has the characteristic bubbly appearance of an astroblastoma (arrow), but a moderate amount of peritumoral T2 hyperintensity associated with the lesion (arrowheads) is present. Furthermore, the cystic component is absent.
B, Axial postcontrast T1-weighted image (550/8) shows the typically intense heterogeneous enhancement of the solid component. The overall imaging characteristics were nonspecific; histologic analysis confirmed the diagnosis of a well-differentiated astroblastoma.
Discussion
Considerable confusion has surrounded the diagnosis of astroblastoma since its original description as a separate glial tumor by Bailey and Cushing in 1924 (2). Since that time, investigators in three large case series (3–5) have tried to delineate unique histologic characteristics for differentiating astroblastoma from other similar-appearing glial neoplasms, including low- and high-grade astrocytic tumors, embryonal neoplasms (ie, primitive neuroectodermal tumors), and ependymomas (6). It is now generally believed that astroblastomas are indeed a distinct type of neoplasm characterized by a constellation of histologic findings, each nonspecific in itself, but when taken together lead to the diagnosis.
Patient demographics can aid diagnosis. Astroblastomas can occur in persons of any age, but in general they are tumors that develop in children and young adults. In two of the large case series, no predominance between the sexes existed, but Brat et al (4) found a strong female predominance.
Radiologic findings may also aid the pathologist in making the diagnosis of astroblastoma. Our retrospective analysis of the radiologic findings in six patients with astroblastoma determined several characteristic features of these tumors. In general, astroblastomas are large, peripheral supratentorial tumors. On MR images, these tumors are cystic and solid lesions, with a characteristic bubbly appearance to the solid component. These lesions have relatively little peritumoral T2 hyperintensity for their large size, which may be related to the lack of local tumor infiltration into the surrounding brain tissue (4). Finally, they have relatively low signal intensity on T2-weighted images and may show slight attenuation on CT scans.
Such imaging characteristics can assist in differentiating astroblastomas from other brain neoplasms. Differentiating histologic characteristics of astroblastoma from those of ependymoma can be difficult; however, the distinction between these two tumors is more obvious radiologically. The majority of ependymomas are infratentorial and generally centered within or adjacent to the ventricles (7, 8). When in the supratentorial compartment, they usually have a cystic component with relatively high signal intensity on T2-weighted images. However, the cystic component is usually simple, and the solid component lacks the characteristic bubbly appearance seen with astroblastoma (9). Usually a moderate amount of peritumoral T2 hyperintensity associated with ependymomas for their size exists that is attributable to a prominent fibrillary component that invades the adjacent brain tissue.
CT and MR imaging depict astroblastomas as distinct from many of the other peripherally based tumors. Anaplastic astrocytomas and glioblastoma multiforme may have a cystic appearance, but this appearance is caused by central necrosis. Notable peritumoral T2 hyperintensity is usually associated with these tumors. Oligodendrogliomas are rare tumors that usually start in the white matter and invade the cortex; they may be large and have foci of cystic degeneration that may appear bubbly. However, nodular or clumped calcifications are present in 70–90% of oligodendrogliomas, in distinction to the punctate calcifications seen in astroblastoma. Pleomorphic xanthoastrocytoma, ganglion cell tumors, dysembryoplastic neuroepithelial tumor, rare supratentorial juvenile pilocytic astrocytomas, and rare supratentorial hemangioblastomas all generally present with a strongly enhancing mural nodule within a single large cyst. Finally, metastases and lymphoma are more solid masses that have a larger amount of peritumoral T2 hyperintensity for tumor size than that of astroblastoma.
Conclusion
In this review of six cases of astroblastoma, several characteristic imaging features were identified. Astroblastomas are generally large, peripheral, solid, and cystic masses with a characteristic bubbly appearance in the solid component and relatively little associated peritumoral T2 hyperintensity for their large size. They have intense heterogeneous enhancement and relatively low signal intensity on T2-weighted images. On CT scans, they may appear slightly higher in attenuation and often have punctate calcifications. These features may assist in the differentiation of astroblastomas from other supratentorial neoplasms.
Footnotes
Presented as an Excerpta Extraordinaire at the 38th Annual Meeting of the ASNR in Atlanta, Georgia, April 2000.
- Received September 14, 2000.
- Accepted after revision December 6, 2000.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}