
Abstract
Summary: The case of a 43-year-old woman with a several month history of severe back pain is reported. CT and MR imaging revealed an intramedullary cystic tumor, which was considered a dermoid cyst or teratoma. During surgery, the tumor was found within the base of the filum terminale and completely resected. Microscopic studies revealed a mature teratoma with an intramural carcinoid nodule. Thirteen-month follow-up after surgical resection showed no evidence of tumor recurrence or neoplasms elsewhere.
The development of carcinoids in mature teratomas is uncommon and rarely occurs within the spinal canal (1–7). Our review of the English-language literature revealed no cases of carcinoid development in an intramedullary spinal teratoma.
Case Report
History
A 43-year-old Caucasian woman presented with a history of increasingly severe back pain of several months' duration. The pain radiated down to her right hip, leg, and ankle and was accompanied by numbness. She denied having left-sided symptoms and bowel or bladder problems. The physical examination revealed diminished range of motion in her back and palpable spasm. She demonstrated a positive Lasègue's sign on the right, indicative of sciatic-type pain. Pin prick resulted in patchy loss of sensation and vibration of the right leg and foot. She did not exhibit hyperreflexia and had a negative Babinski's sign. Her strength was normal in both the upper and lower extremities. A small tuft of hair in the midline of the lumbosacral region of her back was noted.
MR imaging of the lumbar spine revealed a well-circumscribed oval intradural mass posterior to the second lumbar vertebral body. Various components of the lesion exhibited different characteristics. Most of the lesion had increased signal intensity on T1-weighted images (Fig 1A). On T2-weighted images, the lesion was more heterogeneous but had primarily decreased signal (Fig 1B). The hyperintense T1 signal and hypointense T2 signal were consistent with the presence of fat. Within this mass was a mural nodule that demonstrated hypointense signal on T1-weighted images (Fig 1A) and hyperintense signal on T2-weighted images (Fig 1B). This nodule enhanced intensely after the administration of gadopentetate dimeglumine (Fig 1C). The mass was in the right side of the canal and was intimately associated with the conus medullaris, which it displaced anteriorly and to the left (Fig 1D). Within the spinal cord, just proximal to the mass, was a short, centrally located cylindrical structure with signal intensity compatible with cerebral spinal fluid on all images (Fig 1C). This lesion was thought to represent a syrinx or possibly a ventriculus terminalis, a congenital lesion. The heterogeneous nature of the mass and the evidence of fat content were consistent with the MR appearance of the few spinal teratomas described in the literature; however, the hyperintense nodule appeared unique to this case.

Sagittal MR images of the lumbar spine reveal the heterogeneous appearance of the mass indicative of a variety of components.
A, On T1-weighted image, most of the mass is hyperintense (arrowhead) with a hypointense mural nodule (arrow).
B, On T2-weighted image, the mass shows mixed signal intensities (arrow). The cystic lesion within the spinal cord proximal to the mass is quite visible (arrowhead).
C, After administration of gadopentetate dimeglumine, T1-weighted image shows the intense enhancement of the nodular component (arrow).
D, Axial T1-weighted image shows the mass (arrow) within the spinal canal, with leftward displacement of the conus medullaris.
The patient underwent decompressive thoracolumbar laminectomy and excision of the spinal mass thought to be a teratoma or epidermoid cyst. During surgery, an intradural, intramedullary cystic mass attached to the conus medullaris, and filum terminale was noted. The conus medullaris was displaced caudad. The cystic mass was found to be wholly within the base of the filum terminale. The tumor was readily separated from the surrounding spinal cord and was removed as a whole.
The patient's postoperative course was uneventful. By postoperative day 5, she was able to ambulate without assistance and was free of pain, numbness, or weakness. There was no evidence of sphincter dysfunction. Her only neurologic symptom was right leg and ankle numbness, which she had during her initial presentation. Postoperative MR imaging showed no evidence of residual mass. A postoperative cerebrospinal fluid puncture procedure showed no evidence of leptomeningeal dissemination. When last seen 13 months after surgery, the patient was in excellent health. Neuroimaging studies revealed no evidence of tumor recurrence.
Gross examination of the surgical specimen revealed an encapsulated, smooth, tan, soft-tissue mass measuring 3.5 × 2.5 × 2.3 cm. Serial sections revealed a cyst with a firm, pink-tan, mural nodule measuring 1.5 × 1.3 × 1.0 cm. The nodule was attached to the cyst wall by a narrow stalk (Fig 2). The cut surfaces of the nodule were pink-tan without evidence of hemorrhage or necrosis. The rest of the internal surface was yellow-tan and focally covered with yellow, greasy material. The specimen was fixed with 10% neutral formalin and routinely processed. Sections 6-μm thick were cut and stained with standard hematoxylin and eosin; various special stains including periodic acid-Schiff, Alcian blue, and mucicarmine; silver stains including Pascual (argyrophil) and Fontana-Masson (argentaffin) methods; and multiple immunostains. For immunohistochemistry, polyclonal antibodies against nonspecific esterase (NSE), synaptophysin, chromogranin, cytokeratin AE1/AE3, prostate specific acid phosphatase (PSAP), glial fibrillary acidic protein, prostate specific antigen, carcinoembryonic antigen, and thyroglobin were used with ABC vector kits.

Specimen for macroscopic examination shows well-encapsulated soft-tissue mass with a smooth, tan external surface. Cut surfaces show a cystic mass with a mural firm pink-tan nodule that attached to the cyst wall by a narrow stalk. The cut surfaces of the nodule are pink-tan without evidence of hemorrhage or necrosis. The rest of the internal surface is yellow-tan and focally covered with yellow, greasy material
Hematoxylin and eosin–stained sections revealed a cyst predominantly lined by stratified squamous epithelium with some areas of transitional-type epithelium, tall columnar mucinous epithelium with scattered goblet cells (Fig 3A). The nodule was mainly composed of uniformly polygonal cells with finely granular cytoplasm and round to ovoid nuclei with fine chromatin. These cells were arranged in trabecular, solid, insular, glandular, or follicular patterns. There also were scattered dilated glands and transitional-type glands lined by intestinal-type epithelia including goblet cells and columnar and endocrine cells (Fig 3B). The intestinal-type epithelia and amorphous pink or blue material within some of the dilated glands were strongly positive for mucicarmine, Alcian blue, or periodic acid Schiff. Some carcinoid cells contained argyrophil or argentaffin granules as revealed by Pascual and Fontana-Masson stains, respectively (Fig 3C). Foci of squamous differentiation and calcification also were present in the carcinoid tumor. The carcinoid component was entirely contained within the mature teratoma without significant infiltration of the cystic wall. There was minimal nuclear pleomorphism or atypia, and no mitoses were present.

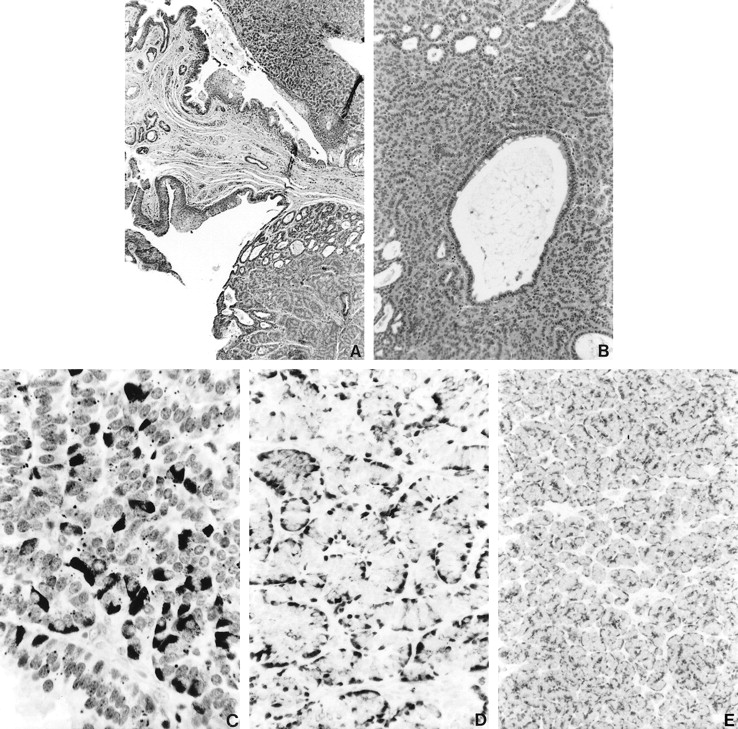
Photomicrographs of a mature cystic teratoma with an intramural carcinoid.
A, Carcinoid component of teratoma shown juxtaposed to cystic wall of teratoma by a narrow stalk (hematoxylin and eosin stain).
B, Mucin-secreting columnar epithelium within carcinoid component (hematoxylin and eosin stain).
C, Carcinoid cells with intracytoplasmic argyrophil granules (Pascual stain).
D and E, Immunohistochemistry shows strong diffuse cytoplasmic positive staining for synaptophysin (D) and weak membrane-like pattern for PSAP in carcinoid (E) (diaminobenzidine chromogen with hematoxylin counterstain).
Most carcinoid cells were immunoreactive for NSE, synaptophysin (Fig 3D), chromogranin, cytokeratin AE1/AE3, and PSAP (Fig 3E) but negative for glial fibrillary acidic protein, prostate specific antigen, and thyroglobin. Some carcinoid cells and cells with squamous or intestinal differentiation were immunoreactive for carcinoembryonic antigen. Cells with squamous differentiation in the carcinoid did not stain for NSE, synaptophysin, or chromogranin. Cells with intestinal differentiation in the carcinoid stained for NSE, synaptophysin, or chromogranin.
Peripheral nerve twigs, columnar epithelia, transitional stratified epithelia, hair follicles, and sebaceous differentiation were identified within the cyst wall. No cartilaginous, bony elements or any immature components within the teratoma were observed.
Discussion
Spinal teratomas are rare lesions composed of a mixture of cell types derived from three germinal layers. On the basis of histologic features, teratomas can be classified into mature, immature, and malignant types. Teratomas can occur at many locations throughout the body including the central nervous system. In the central nervous system, teratomas are rare, constituting approximately 0.5% of mass lesions, and tend to occur in young children, most commonly at midline sites including the pineal body, suprasellar and sellar regions, and the fourth ventricle. Excluding the sacrococcygeal form often seen in neonates, teratomas in the spinal canal are rare, usually developing in the sacrococcygeal region. They might be associated with dysraphic defects (8). Intramedullary spinal teratomas are particularly rare, reported 31 times with two of the cases being immature or malignant teratomas (8).
CT and MR imaging are very useful in suggesting the diagnosis of intraspinal teratoma, as these modalities more readily demonstrate tumor heterogeneity (9). Radiographic features suspicious for carcinoid arising in a teratoma include cystic wall with density compatible with fat and an intramural enhancing or nonenhancing nodule. In this case, MR and CT imaging revealed an intramedullary tumor with a presumptive diagnosis of dermoid cyst preoperatively, although the enhancing mural nodule was thought to be somewhat atypical.
The origin of intraspinal teratomas remains controversial. Poeze et al (8) suggest that intraspinal teratomas might be derived from primordial germ cells misplaced early during embryogenesis, ependymal diverticula of the spinal cord central canal, or a dysembryogenic mechanism. In this case, the patient was noted to have tufted hair on her skin at the sacrococcygeal region, suggesting the presence of associated dysraphic abnormality such as spina bifida occulta. Therefore, misplaced primordial germ cells during embryrogenesis might be a plausible explanation.
Carcinoids arising in teratomas are more difficult to categorize than those developing outside of teratomas. In this case, the histochemical features (both polar positive reactions for argyrophil and argentaffin) and synaptophysin immunoreactivity suggest a midgut origin based on Black's classification of carcinoid neoplasms (10). However, a hindgut origin also is postulated because of the strong PSAP immunoreactivity of carcinoid, as suggested by the work of Kimura and Sasano (11), who have shown that a much higher percentage of carcinoids of hindgut origin express PSAP than those of foregut or midgut origin.
If the tumor is small and nonfunctioning, there are no specific clinical features for carcinoid developing in an intraspinal teratoma, and the presentation is probably identical to cases of intraspinal teratoma or other space-occupying lesions. The symptoms include pain; sensory, motor, and reflex abnormalities of the lower extremities; impotence; paresis; and disturbed sphincter functions of bladder and bowel. Some patients with a large functional carcinoid might exhibit clinical manifestations of carcinoid syndrome. In this case, the patient did not have the clinical signs and symptoms characteristic of carcinoid syndrome.
The prognosis of a carcinoid arising in a mature teratoma within the spinal canal or spinal cord is not known because of the paucity of reported cases, although their biologic behaviors probably are similar to typical intraspinal mature teratomas if the carcinoid has no malignant features. In cases of carcinoid development in a teratoma elsewhere, complete tumor resection resulted in cure in the great majority of cases. In the case reported by Ironside et al (7), the recurrent carcinoid after initial partial resection was resected and further treated with radiation. Significant improvement of clinical symptoms and signs was noted 3 months after surgery, but long-term follow-up was not available. In our patient, no adjuvant radiation therapy or chemotherapy was added after tumor resection, and a good prognosis is predicted because of complete tumor resection and absence of malignant histologic features in the carcinoid or teratoma. The patient is symptom free and without evidence of tumor recurrence or neoplasms elsewhere 13 months after tumor resection.
Acknowledgments
The authors thank Mr. Brent Weedman for preparing the illustrations.
Footnotes
1 Address reprint requests to Mahlon D. Johnson, MD, PhD, Department of Pathology, 113 Nashville Veteran's Administration Medical Center, 1310 24th Avenue South, Nashville, TN 37212.
- Received March 26, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.