
Abstract
Summary: An expansile lesion in the body of the left mandible had high attenuation (225 HU) on nonenhanced CT scans. Histologic examination revealed an odontogenic keratocyst with no evidence of mineralization or calcification within the lesion. The high attenuation was considered to be due to highly concentrated protein of thick, viscous keratin in the lumen of the keratocyst.
Odontogenic keratocysts (OKCs) of the jaw are developmental cysts arising from cell rests of the dental lamina, the oral epithelial lining of the developing tooth follicle. OKCs can be associated with a high recurrence rate, aggressive growth potential, and basal cell nevus syndrome (Gorlin-Goltz syndrome) (1). The lesions have a keratinized epithelial lining (2, 3). On CT scans, the cyst contents usually have low attenuation typical of fluid with a low concentration of protein (4).
Case Report
A 37-year-old man had swelling in the left body of the mandible. A panoramic radiograph showed a well corticated, unilocular, oval radiolucency in the left body of the mandible. Thinning of the inferior cortex of the mandible was present. No resorption of the roots of the teeth or calcification was present in the lesion (Fig 1A).
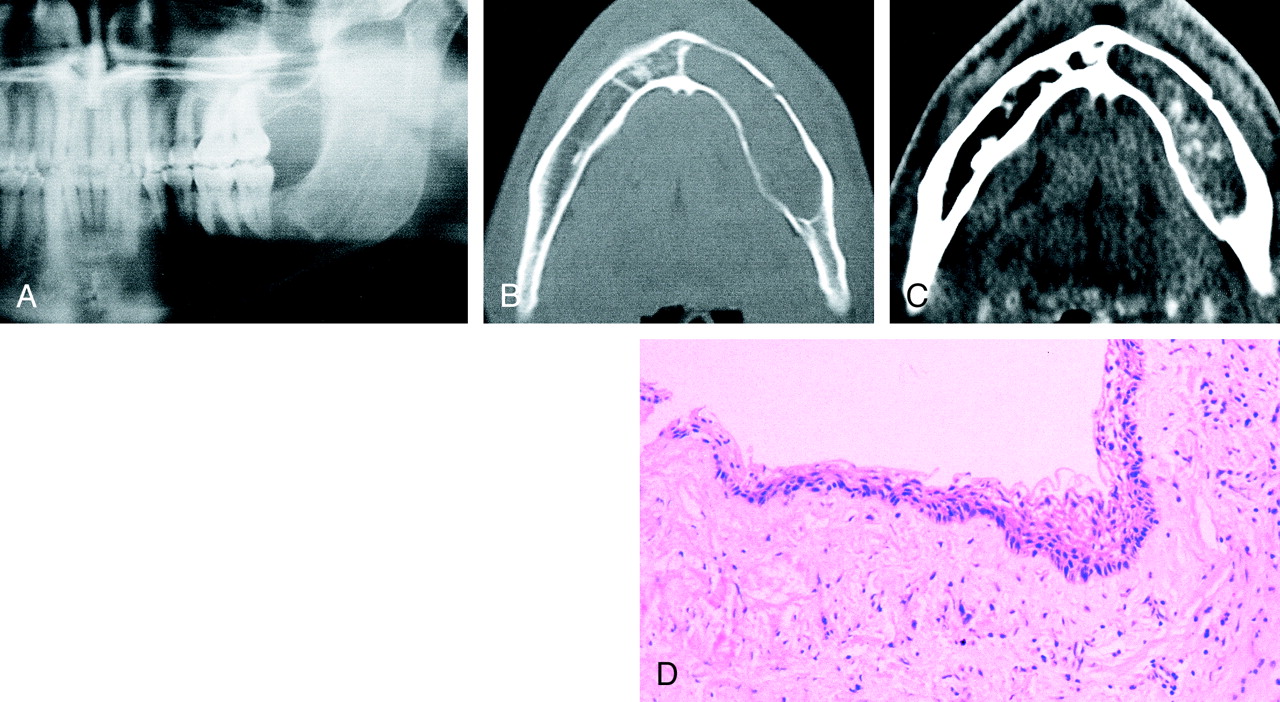
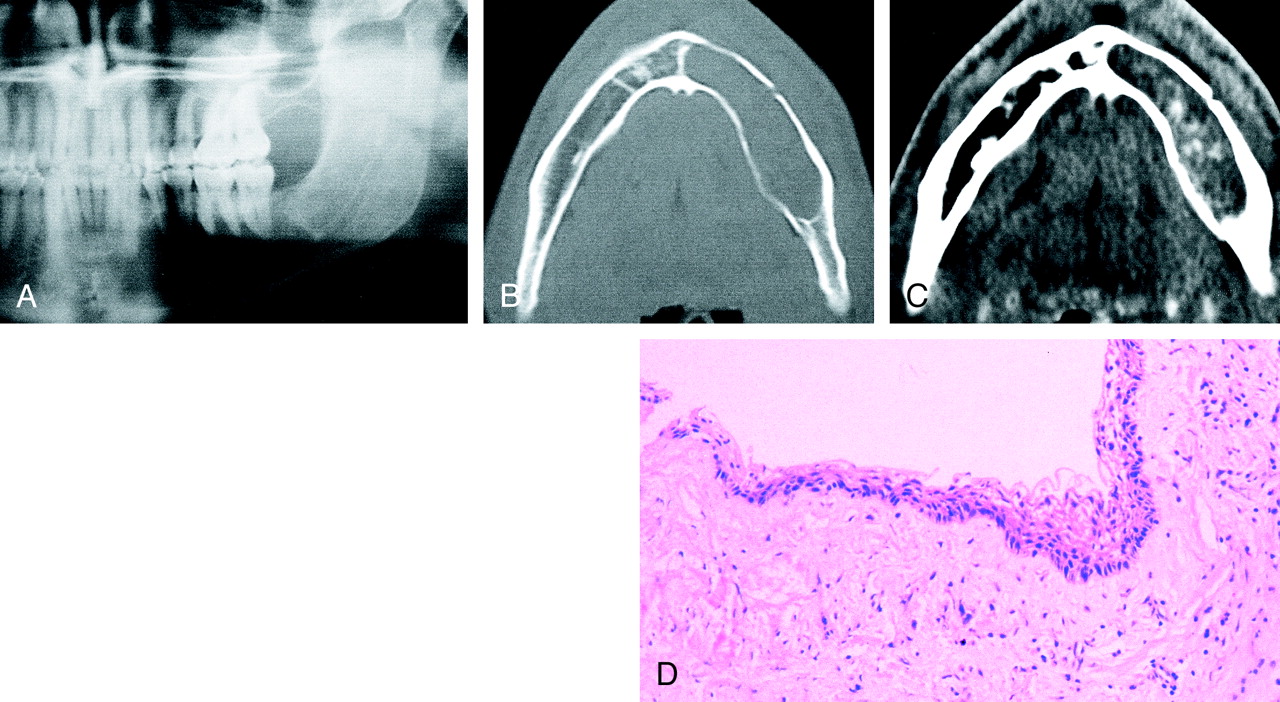
Images show OKC.
A, Panoramic radiograph shows unilocular well-corticated radiolucency in the mandible and thinning of the cortex of the inferior border of the mandible. However, no resorption of roots and calcification in the lesion is present.
B, Axial bone window CT scan shows expansion and thickening of cortex of the mandible.
C, Axial soft-tissue window contrast-enhanced CT scan obtained through the mandible shows high attenuation and expansile abnormality.
D, Photomicrograph reveals a corrugated, wavy epithelial lining of a uniform layer of stratified squamous epithelium. The epithelium is composed of hyperchromatic cuboidal and columnar cells four to six layers thick. Parakeratinized epithelial cells border the lumen.
CT scans obtained with and without contrast enhancement showed an expansile lesion extending from the midline at the symphysis of the mandible to the posterior left molar region. The cortex was expanded, but it was intact and quite thick (Fig 1B). Displacement of the inferior alveolar canal with an intact cortical margin suggested a benign odontogenic lesion (2). The high attenuation (225 HU) in the lesion (Fig 1C) suggested the presence of very-high-density protein or mineralization. If mineralization were confirmed, calcifying odontogenic cyst (Gorlin cyst) or an odontogenic tumor would be considered. No change in the attenuation after contrast enhancement occurred to suggest the presence of a vascularized soft-tissue component (Fig 1C).
The lesion was examined at biopsy, and a decompression stent was placed. The lumen contained a thick, cheesy, yellowish mass of keratin, with no fluid. These findings were macroscopically consistent with those of an OKC. Histologic examination revealed a thin fibrous wall lined with stratified squamous epithelium. The basal layer of epithelium (bordering the fibrous wall) was composed of hyperchromatic cuboidal and columnar cells four to six layers thick. Flattened keratotic epithelial cells bordered the lumen. These findings indicated an OKC (Fig 1D).
The lack of a keratohyaline granular layer and the presence of nuclei within the keratin debris were characteristic of the parakeratotic type of OKC.
Discussion
OKCs are relatively common developmental odontogenic cysts and account for 10–12% of all jaw cysts (3, 5). OKCs usually occur in the second and the third decades of life. Most studies reveal a slight male predominance (1.3:1). Approximately three quarters of all OKCs occur in the body of the mandible, most commonly in the molar region and vertical ramus (3, 5). An OKC usually occurs as a single lesion. Multiple lesions are associated with the nevoid basal cell syndrome (Gorlin-Goltz syndrome) (1). In contrast with other odontogenic cysts, OKCs have a high recurrence rate, reportedly ranging from 13% to 60% (2–7). In approximately 50% of patients, the lesion is asymptomatic. In others, pain, swelling, expansion, drainage, and bone perforation are reported (2, 5).
At histopathologic examination, an OKC has a fibrous wall lined by epithelium with a thin layer of stratified squamous epithelium. This epithelium has a basal layer six to eight cells thick and a lining of flattened keratotic epithelial cells. The formed keratin lines the luminal surface of the epithelial cells in a slightly wavy or corrugated pattern (2, 3). The luminal content can have different consistencies described as a “straw-colored fluid”; “thick puslike” material; or a caseous, thick, cheesy, milk-white mass (2, 4). The varying consistencies reflect various densities of keratinacious debris.
At histologic examination, OKCs have been classified by some authors into parakeratotic and orthokeratotic subtypes (5, 7). These types refer to the histologic characteristics of the lining and the type of keratin produced. Compared with the parakeratotic subtype, the orthokeratotic subtype produces keratin more closely resembling the normal keratin produced by the skin. A keratohyaline granular layer is immediately adjacent to the layers of keratin. The keratin (orthokeratin) does not contain nuclei. The parakeratotic subtype has a more disordered production of keratin. No keratohyaline granules are present, and cells slough into the keratin layer. The keratin contains nuclei and is referred to as parakeratin. The parakeratotic type is the most frequent (80%) and has a more aggressive clinical presentation than the orthokeratinized variant (2–4). Some pathologists think that the orthokeratotic subtype should be classified as a separate entity and called an orthokeratotic odontogenic cyst, because of the histologic features and is substantially less aggressive behavior. The lesion reported in this article is a typical parakeratotic OKC.
At surgery, an OKC is usually described as having a thin friable lining. The most frequently recorded gross feature is the presence of fluid with cheesy or caseous material filling the cystic lumen. These characteristic features often enable the diagnosis of OKC during initial examination of the gross surgical specimen, before histologic examination (2). The gross findings in this report were consistent with those of a parakeratotic OKC.
The following radiographic features are characteristic of OKCs: 1) a distinctly corticated, often scalloped, border; 2) expansion, especially toward the lingual (medial) side, and growth along the length of the mandibular bone; 3) displacement of developing teeth and/or separation or resorption of the roots of erupted teeth and extrusion of erupted teeth; 4) a radiolucent lumen, and occasionally a cloudy or milky appearance of the lumen on the panoramic radiograph; 5) the occasional presence of multiple or bilateral cysts, suggestive of basal cell nevus syndrome (5, 8, 9).
CT provides additional information about the contents of the lesion. The high attenuation in this case is thought to be the result of a high protein concentration in the dense keratin filling the lumen. Other possibilities could include hemorrhage or calcification.
If the high attenuation represented calcification rather than simply a high protein content, the differential diagnosis would include a Gorlin cyst (calcifying odontogenic cyst), Pindborg tumor (calcifying odontogenic tumor), and adenomatoid odontogenic tumor (5, 8, 9). Calcification was not found at the histologic examination in the present case.
High attenuation on CT scans also could have been caused by blood. A hemorrhagic bone cyst (simple bone cyst) should be included in the differential diagnosis. A vascular lesion or malformation also should be considered. However, with a vascular lesion, a change in attenuation should occur when a contrast-enhanced CT scan is compared with a nonenhanced CT scan.
The difference in attenuation is unlikely to help in the distinction between the typical parakeratotic OKCs and the less aggressive orthokeratotic subtype of odontogenic cysts. Yoshiura et al (4) noted varying attenuations in both types of lesions. The attenuation did not help in the differentiation. Most parakeratotic keratocysts have low attenuation within the lesion (10). The case described in this report had a high attenuation of 225 HU. Therefore, either type of cyst may have high or low attenuation.
On MR images, an OKC typically has low to intermediate signal intensity on T1-weighted images and high signal intensity on T2-weighted images. This pattern may be caused by fluid containing a low concentration of protein, which results in intermediate signal intensity on T1-weighted images. Minami et al (9) reported that 13 (68%) of 19 OKCs had this typical pattern. Four (21%) had a mixed pattern with areas of high to intermediate signal intensity on T1-weighted images and low signal intensity on T2-weighted images mixed with the more typical pattern (high signal intensity on T2-weighted images). Two lesions had uniformly intermediate signal intensity on T1-weighted images and low signal intensity on T2-weighted images. The areas of low signal intensity on T2-weighted images are consistent with a solid component or high protein concentration (11). The more solid components in the six lesions showed no enhancement. Thus, it is unlikely that this finding represented solid vascularized tumor. The findings are more consistent with highly protenacious or desiccated secretions such as thick keratin debris.
In summary, high attenuation within an expansile benign lesion of the mandible on nonenhanced CT scans, with no enhancement after contrast material injection, can indicate an OKC. The high attenuation suggests the presence of a dense proteinacious material such as keratin.
Footnotes
1 Address reprint requests to Hugh D. Curtin, 243 Charles Street, Boston, MA 02114.
References
- Received February 23, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.